
Intractable Plantar Keratoma (IPK) is one of the most common problems seen in the foot. Plantar means the bottom of your foot. Keratoma is a hard, thickened portion of skin. An IPK is associated with abnormal pressure caused by a misaligned bone. Intractable plantar keratosis also is known as plantar callus and calvus durusm is a rare and painful condition for both men as well as women which is caused by the accumulation of the dead skin cell over the hard thick part of our foot. There are several treatments been adopted for this thing but all have their limitations, treatments like Keratosis including regular trimming, acid clearance and cyro therapy verrucous carcinoma, epidermal inclusion cyst and also old surgery Due to their unique presentation, intractable plantar keratosis can be challenging to treat and can be particularly very painful. This author reviews the biomechanical causes of intractable plantar keratosis, offers pearls on making a diagnosis, and provides a guide to surgical techniques for various iterations of the condition.
Cause of this condition

This condition is mostly caused by dropped metatarsal, which happens when the metatarsal head drops to some lower level than the surrounding metatarsals and protrudes from the bottom of the foot. Once that drop occurs, more pressure is applied to the protruding area and causes a thick centralized callus to form which is known as IPK. It is also said that IPK would not just appear overnight to us. If you have one metatarsal bone that is longer or lower than the others it will be hitting the ground first which causes it to sustain more force than it is used to handle. This, in turn, will eventually lead to the development of an IPK that is centralized around the area receiving the unwanted pressure. or a sub-second lesion due to a hypermobile first ray. These are the true etiologic components of the intractable plantar keratosis, not the lesser metatarsal. The component surgeons often overlook is the relationship of equinus to intractable plantar keratosis formation. Equinus is directly related to hypermobility of the first ray and pronatory changes of the foot, which can result in flexor stabilization hammer digit formation. Additionally, equinus causes increased loading of the forefoot, resulting in elevated peak pressures.
This sensation of having an IPK is sometimes compared to walking on a stone that you simply cannot kick out of your shoe. In most cases, a dropped metatarsal is caused by a congenital abnormality, a result of a metatarsal fracture, or a structural change that may have occurred over time.
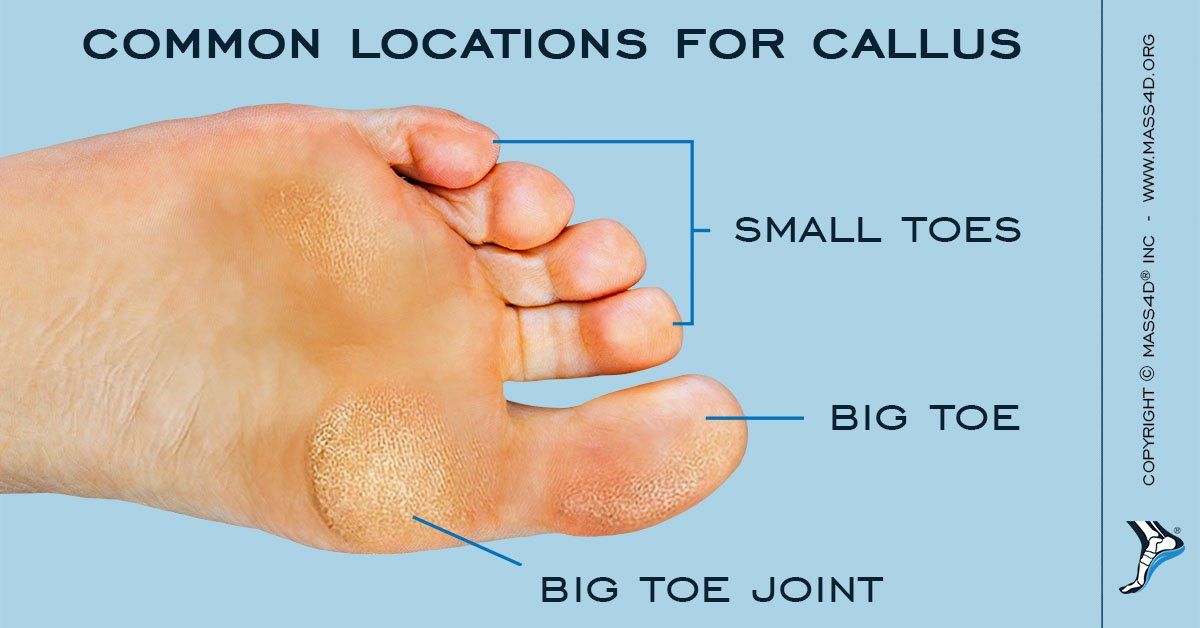
Although they can sometimes be mistaken for an ordinary callus due to their similar appearance and location, an Intractable Plantar Keratoma is far more painful and harder to ignore due to its location deep under the ball of the foot.
No matter what, I believe you must treat the underlying etiology as well as the symptoms. In the case of intractable plantar keratosis, there is the symptomatic dermatologic lesion and the underlying etiologic pathologic conditions. To be clear, the vast majority of these have nothing to do with the lesser metatarsal.How can it be treated?
It can be treated non-surgically when there is no associated rigid digital hammertoe deformity. Some like to treat the dermatological condition with topical 40% salicylic acid pads and debridement. Typically, the intractable plantar keratosis will resolve in three to four weeks of treatment. If equinus is present, one must also address this with dorsiflexion bracing for one hour per day, usually for two to three months. Finally, one must treat any underlying biomechanical deformity. Use custom orthoses to treat a pronatory pathology associated with intractable plantar keratosis formation. Examples of pronatory pathologies would be a sub-second metatarsal lesion due to a hypermobile first ray or flexible hammer digit syndrome. One may treat semi-rigid hammer digit syndrome through digital splinting.
Surgical intervention becomes much more likely when there is an associated rigid hammer digit to the intractable plantar keratosis. You can treat the lesion and the equinus either surgically or non-surgically. One must treat all components for a successful resolution. The metatarsal parabola is critical regarding forefoot biomechanics and proper maintenance will best serve you and your patients. Podiatric surgeons can treat intractable plantar keratosis conservatively under the right circumstances. The key to successful conservative resolution is treating the symptomatic dermatologic lesion and the underlying etiologic lesion. By carefully examining the underlying pathologies, one can achieve consistent results without a metatarsal osteotomy, which one should reserve for a truly plantarflexed or elongated metatarsal.
Conclusion
Rather than just assuming the intractable plantar keratosis is due to a long metatarsal or plantarflexed metatarsal, physicians should evaluate the condition globally concerning the arch type, concomitant deformities, and biomechanical influences. Don’t forget to have the patient get out of the treatment chair and walk for you to assess his or her gait. Hopefully, a treatment that addresses functional faults and structural deformities will lead to good outcomes for your patients with resolution of pain and accompanying intractable plantar keratoses.

No